
Tox Files: Hyperthermic Emergencies
and an introduction to dr. justin arnold, our favorite toxicologist
It is my pleasure to bring you a toxicology post and just in time for Halloween! This is based on a patient experience that could have been a scene from Tales from the Crypt. If you’re too young to know what the heck I’m talking about, please check out Tales from the Crypt on Netflix this Halloween Season! The patient was seen by myself and resident physician, Dr. Bryan Hyman. Coincidentally, just a few weeks prior to taking care of this patient we had listened to a great lecture by our home toxicologist and leader of our poison center, Dr. Justin Arnold. Let’s review the case and some of the key pearls. I’ve also included Dr. Arnold’s toxicology lecture on hyperthermic emergencies as well as a brief interview with him to share with our readers.

A few minutes prior to change of shift a patient triaged as “psychiatric clearance” arrived. I was the oncoming night physician.
7:00pm sign out – “Room number 10 just arrived for psychiatric clearance. She has a history of psychosis on ziprasidone and came in acutely agitated and altered. We can’t send her to psychiatric facility because her white count is 30 for unknown reason. She’s completely manic and difficult to control so we haven’t been able to really dig into what’s going on yet. She likely needs head CT and infectious work up. Unfortunately, she just returned from CT scanner prior to scan being completed because she’s so agitated despite a dose of haldol.”
Our initial evaluation – Patient is actively having psychotic hallucinations and talking nonsensically, writhing around in bed. HR 120, BP 150 systolic. She is diaphoretic with foamy secretions coming from mouth. No clonus or significant rigidity appreciated on initial exam but difficult to fully assess tone because patient resist exam and is constantly attempting to move. Rectal temp obtained, 101.5.
“It’s not a good day for your patient when tetanus and rabies actually make it onto your list of differential diagnoses.”
Differential: sepsis, meningitis, encephalitis, thyroid storm, neuroleptic malignant syndrome, delirium tremens, serotonin syndrome, drug intoxication, toxicologic cause, tetanus, rabies, pheochromocytoma, other.
The Game Plan: Broaden work up (full infectious work up with all the normal things as well as CSF studies, CPK, thyroid studies, ammonia), cover empirically with antibiotics and acyclovir, calm agitation with benzos, get the head CT, attempt LP, and admit.
How Things Really Went: The patient was monitored closely at bedside with end-tidal CO2 monitoring. We gave multiple doses of escalating benzodiazepines (think 10mg of haloperidol, 2 mg of IV lorazepam x 2, 10 mg of IV midazolam) with little improvement in her severe agitation. She became progressively more altered with legit psychosis, more diaphoretic, and had ongoing tachypnea despite our benzos. She was untouched by our medications and in a psychotic rage requiring restraints. We triple checked to make sure her IV was working- it was. Ultimately, we had to intubate and sedate her using etomidate and rocuronium. Sedation following intubation remained a challenge due to unpredictable autonomic swings in her vitals. Her heart rate and blood pressure had wide fluctuations anywhere from HR of 100-170. Her BP fluctuated back and forth from hypertensive to hypotensive requiring pressors. At times she was requiring both a versed and propofol drip to try and keep her comfortable.
She was admitted to the ICU for presumed sepsis with neuroleptic malignant syndrome on our differential. Neurology was consulted and felt her condition was concerning for NMS. Her blood cultures later returned positive for MSSA of unclear etiology. The remainder of her laboratory work up was remarkable for a metabolic acidosis. She did not receive Dantrolene or Bromocriptine. She was able to be extubated on hospital day 3 and recovered. This patient doesn’t fit the diagnosis of NMS perfectly. Most notably, she did not demonstrate true leadpipe rigidity at the time of my initial exam but her condition did seem to worsen. Common things being common, this may have simply been severe sepsis with acute delirium or some other multifactorial condition such as sympathomimetics + sepsis. NMS generally presents with severe lead pipe rigidity and higher initial temperatures. The recovery period for NMS is usually much longer than what this patient experienced. Though sepsis and encephalopathy may better explain this patient’s condition, its a great opportunity for us to review NMS!
Review of NMS
History & Symptoms:
Recent Dopamine Antagonist causes altered hypothalamic set point. Haldol most commonly. Usually therapeutic dosing exposure rather than OD. Evolves over days/weeks. Note that NMS may also be caused due to withdrawal of a dopaminergic medication.

The Exam
Muscle rigidity - generally severe
Hyperthermia > 38 C on 2 or more occasions
Other possible findings:
Autonomic dysfunction: hypertension or labile BP fluctuation, tachycardia, tachypnea, diaphoresis
AMS
Tremor
Differential:
Review the broad differential in our initial management. Dr. Arnold’s lecture included these tox specific differentials to include in hyperthermic patients:
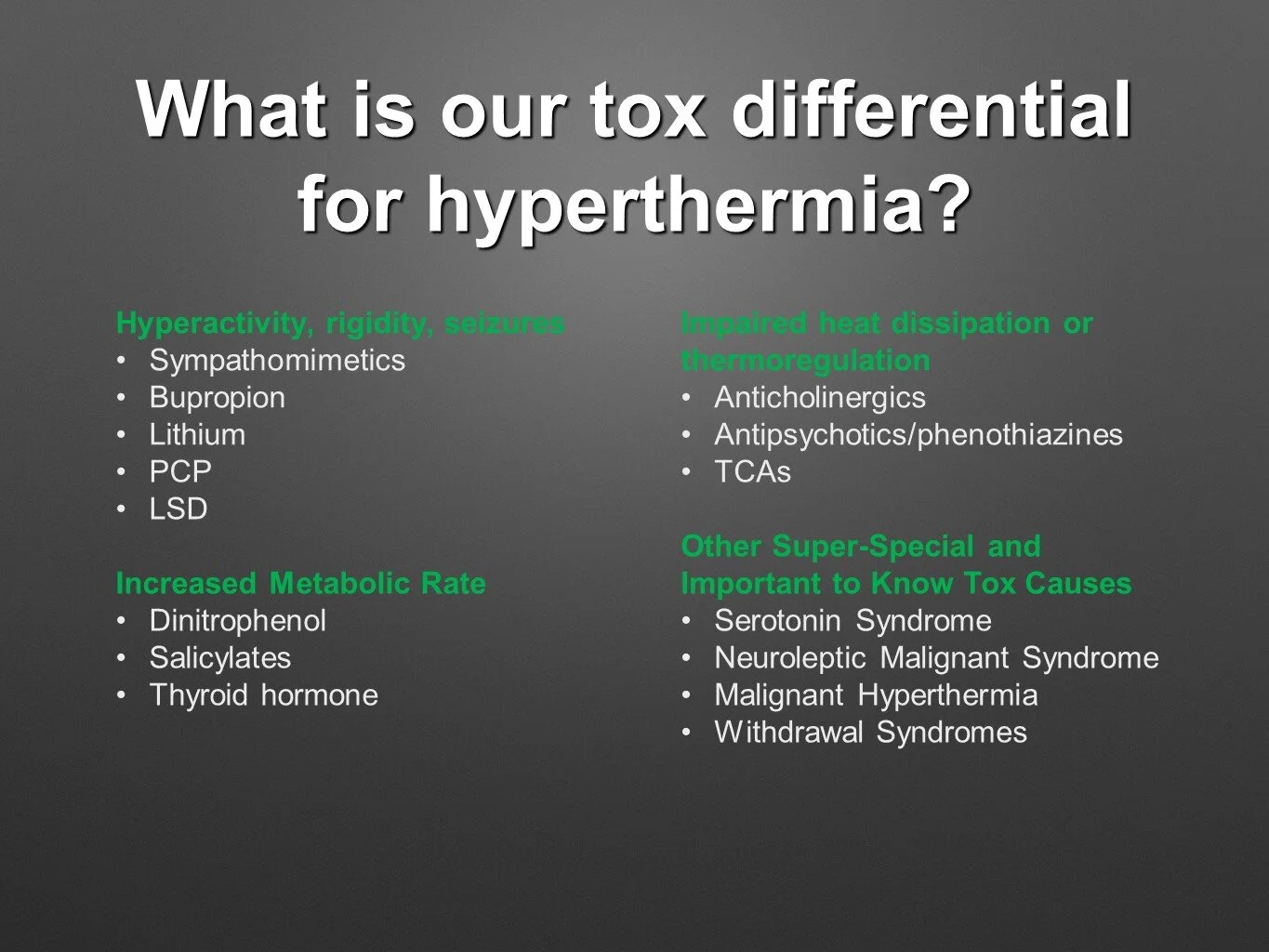
Slide taken from Dr. Arnold’s Presentation, “It’s Hot in Here,” September 16, 2020.
Work up:
Shout out to PEPID for making my life on shift easier! This is a good place to start with your initial work up.

Image Courtesy of Pepid EM Platinum
Treatment:
#1) Benzodiazepines!
Aggressive Supportive Care
Non-depolarizing paralytic if intubation required
Consider Dantrolene – unclear if beneficial but some sources support the use.
Consider Bromocriptine – may have some benefit though the evidence is not great and it requires an oral or NG route of administration.
How can you differentiate NMS from Malignant Hyperthermia or Serotonin Syndrome?
1) History!
Malignant Hyperthermia patients have a history of anesthesia and generally develops quickly.
NMS must have exposure to neuroleptic medication or withdrawal of dopaminergic medication. Onset is generally more gradually and progressive.
Serotonin Syndrome also has a specific group of medications that you should consider and patients will have hyperreflexia and clonus
check out this lecture on toxicologic hyperthermic emergencies!
Meet the EM Physician Leading Our Poison Center

Chatting with Dr. Arnold
When did you develop your interest in toxicology?
As a resident I was privileged to do a toxicology rotation with J. Ward Donovan, MD at Pinnacle Health in Harrisburg, PA. Dr. Donovan was a legend in toxicology and made it my most memorable month in residency.
What's an average day like in the life of an EM toxicologist at Tampa General?
As the Medical Director for our Poison Center, much of my day is split between clinical and administrative duties at the Poison Center and teaching. I spend a lot of time reviewing cases at the poison center, talking with our Poison Specialists and other physicians, developing guidelines, and teaching our residents, medical students, and pharmacy students. I really love the time teaching – it’s my favorite part of what I do every day!
What's your favorite toxicology topic?
This is a hard one. I really love critical care toxicology such as calcium channel blocker and bupropion ingestions. I also love natural toxins like snake and marine envenomations as well as poisonous plants and mushrooms.
Any plans of expanding the TGH program or starting a fellowship?
We actually just added another Medical Toxicologist to our staff and as we continue to add more we hope to start a robust inpatient consult service and someday a Medical Toxicology Fellowship.

What strange toxicology related items line his office shelf?
Toxicologists are notorious for having strange collections and bizarre chemistry related equations adorning their offices. What oddity is in your office?
I’m no exception to this. One of the strangest things in my collection is probably homemade moonshine that is contaminated with the 2nd highest concentration of lead reported. This belonged to a couple I treated in the hospital for lead poisoning while in fellowship and I actually obtained it by going to their house.
What is the biggest advantage of taking a toxicology rotation at USF?
Residents rotate at the Poison Center which is directly across the street from the ED. We have a robust toxicology faculty group. Our teaching emphasizes current poison control cases involving critically ill patients and a good variety of uncommon exposures. Residents see a breadth of pathology that is unlikely to be seen at a single hospital. Our residents leave the rotation comfortable in managing most poisonings, overdoses, and envenomation that would present to their ED.
What's your favorite non-work related activity in Tampa?
I’m a big fan of anything to do with the ocean. Specifically, I love boating with my family and fishing inshore, nearshore, and offshore with my friends.
References
Perry PJ, Wilborn CA. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry. 2012 May;24(2):155-62. PMID: 22563571.
Berman BD. Neuroleptic malignant syndrome: a review for neurohospitalists. Neurohospitalist. 2011;1(1):41-47. doi:10.1177/1941875210386491
Bradley J, Ellingson C, Ballarin D. PEPID Review of Neuromalignant Syndrome. Updated 2019 Jan.
Arnold J. It’s Hot in Here. USF Grand Rounds Sept 2020.
about the author
Dr. Okonkwo is the Assistant Program Director at USF. She attended medical school at Indiana University and completed her emergency medicine residency training at Carolinas Medical Center in Charlotte, North Carolina.