
Hip Dislocations with Dr. Gerges
Hip dislocations… when should you reduce, and when should you call for help from the big guys? (More often that not, quite literally, the big guys. No offense to the awesome female orthopedic surgeons out there!)
This is one of the things we will discuss today during our talk about this rare but frankly debilitating orthopedic emergency. When you hear the words “hip dislocation,” you probably picture an elderly person after a ground-level fall. But unfortunately, younger people who are involved in MVCs, involved in high energy contact sports, or sometimes even just falls from height can present with the very same problem. In this quick talk, we will tackle the most time sensitive challenges that occur whenever a hip dislocation patient presents to your ER.
Avascular Necrosis
Keep calm! You have a six-hour window from the time of the hip dislocation to reduction to decrease the risk of avascular necrosis of the femoral head.
Well, don’t keep calm too much. But if you’re within that six-hour window and decide to reduce the hip, don’t forget to give enough Propofol to get adequate muscle relaxation to increase your chances of a successful reduction. Even more importantly, do not forget to do your neurovascular exams before and after the reduction!
The six-hour rule for reduction does not apply to prosthetic hips, since there is no salvageable femoral head that you have to worry about.

Concurrent injuries
With the posterior dislocation that often occurs with flexed knees accompanied by axial loads, make sure you don’t miss acetabular fractures, sciatic nerve injuries, or other joint injuries--especially the knee.
Anterior dislocations can cause femoral head impactions, but they are much less common than posterior hip dislocations.
Acetabular fractures can be subtle, so you don’t want to miss them-
The blue, black and red arrows represent the normal iliopectineal line, ilioischial line and acetabular teardrop.
But look at where the pink arrow points. It shows loss of congruence and loss of the smooth contours you can find on the opposite side (where the blue arrows point).
Also, you can see that the ilioischial line (white arrow) does not bisect the acetabular teardrop (red arrow) like it does on the left hip (black arrow).
All of this points to an underlying acetabular fracture on the patient’s right side.

Management
Reduction
Within 6 hours for the native hip
Do NOT reduce if there is a concomitant femoral neck fracture, it’s a strict contraindication.
Operative fixation
Delayed presentation after 6 hours from the time of dislocation
Unsuccessful reduction attempts
Femoral head, neck or acetabular fracture--call Ortho promptly if any of these are present.
The Reduction Techniques
Captain Morgan
Put provider’s knee behind patient’s flexed knee
Apply anterior force and lift your knee up as hard as you can

Waddell technique
Provider on patient’s bed
Place forearm under the patient’s knee
Squat down, apply posterior traction with the full force of your body while stabilizing your elbow on your knee.

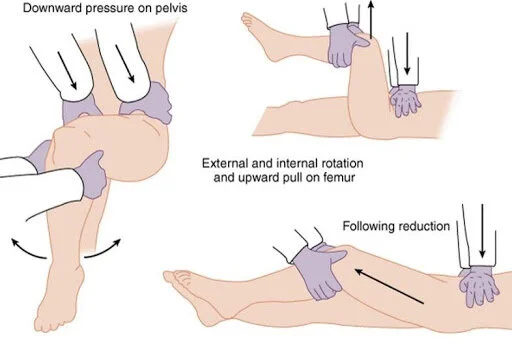
Allis Maneuver
Firm distal traction at flexed knee to pull head back into acetabulum assistant stabilizes pelvis by
pushing on ASISs
About the author
Dr. Marco Gerges is a first year resident with the University of South Florida Emergency Medicine program at Tampa General Hospital
Edited by Dr. Michael Weaver